- Grant: FC 008/2015
- Title: Vitamin D and celiac disease (VitaCeD)
- Topic: Celiac Disease, Clinics
- Duration: Triennial Project
- Principal Investigator: Prof. Carolina Ciacci, University of Salerno
- Partnerships:Fabiana Zingone (University of Padua); Paola Iovino (University of Salerno); Antonella Santonicola (University of Salerno); Ilaria Russo (University of Salerno); Najla Hajji (University of Salerno); Carlotta Ruocco (University of Salerno)
Publications originated from the Project:
- Zingone F, Iovino P, Bucci C, Ciacci C. Coeliac disease: no difference in milk and dairy products consumption in comparison with controls. BMJ Nutr Prev Health. 2019 Mar 19;2(1):39-42. doi: 10.1136/bmjnph-2018-000022. PMID: 33235956; PMCID: PMC7678477. https://pubmed.ncbi.nlm.nih.gov/33235956/
- Vitaglione P, Zingone F, Virgilio N, Ciacci C. Appetite and Gastrointestinal Hormone Response to a Gluten-Free Meal in Patients with Coeliac Disease. Nutrients. 2019 Jan 3;11(1):82. doi: 10.3390/nu11010082 https://pubmed.ncbi.nlm.nih.gov/30609862/
- Ciacci C, Bilancio G, Russo I, Iovino P, Cavallo P, Santonicola A, Bucci C, Cirillo M, Zingone F. 25-Hydroxyvitamin D, 1,25-Dihydroxyvitamin D, and Peripheral Bone Densitometry in Adults with Celiac Disease. Nutrients. 2020 Mar 27;12(4):929. doi: 10.3390/nu12040929 https://pubmed.ncbi.nlm.nih.gov/32230847/
- Zingone F, Ciacci C. The value and significance of 25(OH) and 1,25(OH) vitamin D serum levels in adult coeliac patients: A review of the literature. Dig Liver Dis. 2018 Aug;50(8):757-760. doi: 10.1016/j.dld.2018.04.005 https://pubmed.ncbi.nlm.nih.gov/29773507/
THE STUDY
Project rationale
The existing literature on vitamin D level in Celiac Disease (CeD ) presents several limitations. For example, most studies rely on a limited number of patients, rarely taking into account the possible cofactors influencing vitamin D level, such as sun exposition, age, type of diet, type of laboratory test used in the study, etc. However, the main limitation is that only a few reports analyze the calcitriol plasma levels in CeD. According to most scientific societies and researchers, vitamin D deficiency occurs when the serum 25(OH) vitamin D concentration is below 30 nmol/L (12 ng/ mL). However, different epidemiological and clinical studies use different assays, with a variation that can reach up to 25% in the section of the population needing treatment for vitamin D deficiency. The difference in the standard may have affected also the literature regarding CeD.
A recent review (paper 1) indicates that most of the studies on vitamin D in CeD report 25 (OH) vitamin D deficiency at diagnosis that disappears on a gluten-free diet, independently of any supplementation, whereas when the calcitriol, the 1,25 (OH) vitamin D, was evaluated, it resulted high at the time of CeD diagnosis. However, it is object of scientific debate which is the role of dietary calcium and calories intake, vitamin D malabsorption, and/or the inflammatory status due to the gluten contact in determing low BMD in CeD.
Aims:
1. to study patients with untreated or treated CeD for:
- a) collection of clinical records and dietary assessments and GFD compliance
- b) to measure plasma 25-hydroxy vitD and 1,25-dihydroxy vitD levels and ions indices of mineral metabolism and parathyroid gland activity.
- c) to measure the bone mass/bone density by pQCT and its correlation with the above mentioned indices
2. to study in-vitro by the means of the organ culture of intestinal biopsies in active and treated CeD the separate effects 25-hydroxy vitD and of 1,25-dihydroxy vitD on early immunologic/inflammatory events after in vitro gliadin challenge
Experimental design and methodologies
- Review of the literature
- Investigation on the dietary habits of our population
- Study of bone mass and vitamin D levels
Research plan and results obtained
1. Review of the literature
Within the wide spectrum of symptoms and alteration of systems that characterizes CeD, several studies indicate a low-level of vitamin D, therefore recent guidelines suggest its evaluation at the time of diagnosis. This review examines the data from existing studies in which vitamin D has been assessed in CeD patients. Our review indicates that most of the studies on vitamin D in adult CeD report a 25 (OH) vitamin D deficiency at diagnosis that disappears when the patient goes on a gluten-free diet, independently of any supplementation. Instead, when the calcitriol, the active 1,25 (OH) vitamin D form, was evaluated, it resulted in the normal range at the time of CeD diagnosis. A strict and lifelong gluten-free diet can help recover vitamin D level without any supplementation.
Results published: Fabiana Fabiana Zingone, Paola Iovino, Cristina Bucci, Carolina Ciacci. Coeliac disease: no difference in milk and dairy products consumption in comparison with controls. BMJ Nutrition and Health 2019
2. Dietary habits
Dietary habits: Calcium intake
The damaged intestinal mucosa in coeliac disease may cause lactose intolerance. Celiac patients on a gluten-free diet frequently claim lactose intolerance and therefore avoid milk and dairy products. The hypothesis is made that low intake of dietary calcium may compromise bone mineral density in celiac disease. We examined the average consumption of milk and dairy products and the reasons for not consuming them. An online survey was sent by email to patients with coeliac disease on a gluten-free diet and aged 18–75 and to matched controls were selected among volunteers who responded to the survey posted on the public access sites. 176 patients with coeliac disease and 528 controls participated in the study. We found that 22.2% of the patients with CeD and 19.9% controls do not drink fluid milk on a regular basis. Lactose-free milk is chosen by 20.4% of patients with CeD and 19% of the controls. In our study we describe that there is no significant difference between patients with coeliac disease and controls in regular milk consumption. Follow-up visits for patients with coeliac disease could avoid unnecessary dietary restrictions.
Results published: Fabiana Fabiana Zingone, Paola Iovino, Cristina Bucci, Carolina Ciacci. Coeliac disease: no difference in milk and dairy products consumption in comparison with controls. BMJ Nutrition and Health 2019
Dietary habits: Appetite and Gastrointestinal Hormone Response to a Gluten-Free Meal
Pre-prandial hypoglycaemia, reduced availability of glucose for metabolism and a decreased level of body carbohydrate stores or liver glycogen are stimuli for increased food intake This study aimed to evaluate the post-prandial appetite sensations induced by a mixed meal in patients with CeD at diagnosis (CeDD) and on a GFD (CeDGF) and to clarify the role of GI hormone response. We found that in the post-prandial phase CeDD showed a sustained hunger sensation and a reduced response of plasma GIP and insulin compared to CeDGF and HS. In CeDD, the lower hunger reduction could be explained by the lower GIP response than in CeDGF and HS, in association with the lower GLP-1 than HS. Indeed, GIP and GLP-1 delay gastric emptying at physiological concentration. Therefore, a lower response of GIP in CeDD, in addition to the low GLP-1 level (as in CeDGF vs. HS), could determine a faster gastric emptying and, in turn, a faster returning of hunger. The ghrelin response recorded over time in the three groups were similar and confirmed the previous evidence that the delayed gastric emptying in CeD patients was not associated with reduced ghrelin levels. Data suggested that patients with CeD have an impaired glucose absorption after more than 12 months of gluten-free diet. Postprandial GIP may play a significant role in appetite cues and insulin response to a complex meal.
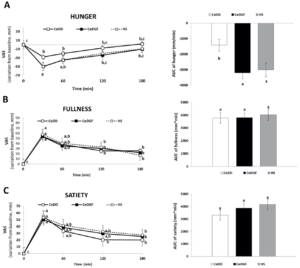
Results published: Paola Vitaglione, Fabiana Zingone, Nicolina Virgilio and Carolina Ciacci. Appetite and Gastrointestinal Hormone Response to a Gluten-Free Meal in Patients with Coeliac Disease. Nutrients 2019
Bone mass and Vitamin D levels
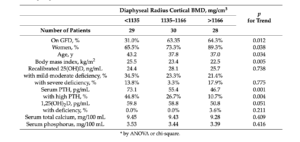
The present study aimed to investigate the serum levels of 25(OH)D and 1,25(OH)2D, minerals, and PTH in adult patients with untreated or treated CeD and to evaluate the correlation of these markers to peripheral BMD as assessed by pQCT. Complete data were collected in 105 patients for lab tests and 87 patients for bone mineral mass (BMD). For lab tests, untreated CeD differed from treated CeD for 22.0% lower serum 25(OH)D (p = 0.023), 42.5% higher serum PTH (p < 0.001, Figure 1), and 13.0% higher serum 1,25(OH)2D (p = 0.029) in the presence of similar serum calcium and phosphorus (p > 0.35). For BMD, Table 1 shows that untreated CeD differed from treated CeD for lower diaphyseal cortical BMD (1133 and 1157 mg/cm3, p = 0.004) but not for distal BMD (total, trabecular, and subcortical, p > 0.13). Independent correlates of diaphyseal cortical BMD were GFD treatment and body mass index (p < 0.05).
Potential pitfalls and caveats
The main difficulty encountered in the study was the in vitro evaluation of the vitamin D forms effect on the intestinal mucosa. Our results, from experiments performed in over 50 biopsy’s samples of patients indicate a pro-inflammatory effect of both forms of Vitamin D in different concentrations, also in its commercially available pharmaceutical forms. The present finding are in contrast with most of the available data and deserve further investigations.
Conclusions:
Data indicated that, compared to CeD patients on a gluten-free diet, untreated adult CeD patients at diagnosis had lower 25(OH)D, higher PTH, and higher 1,25(OH)2D in the absence of difference in serum calcium and phosphorus. 25(OH)D and 1,25(OH)2D, even below the normal range, were not associated with BMD. Our findings do not support the use of vitamin D supplementation for all CeD adults.
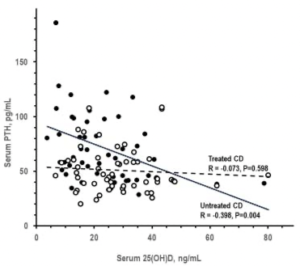
Legend to Figure: Pearson correlation between serum 25(OH)D and serum parathyroid hormone (PTH) in untreated CeD and treated CeD (closed and open symbols, respectively).
Table 1 Analysis by tertile of diaphyseal radius cortical BMD: Prevalence or mean of gluten-free diet (GFD), sex, age, body mass index, and serum concentrations of 25(OH)D, PTH, 1,25(OH)2D, calcium, and phosphorus.
Results published: Carolina Ciacci, Giancarlo Bilancio, Ilaria Russo, Paola Iovino, Pierpaolo Cavallo, Antonella Santonicola, Cristina Bucci, Massimo Cirillo and Fabiana Zingone. 25-Hydroxyvitamin D, 1,25-Dihydroxyvitamin D, and Peripheral Bone Densitometry in Adults with Celiac Disease. Nutrients 2019